No two people experience obesity in exactly the same way, especially in kids and teenagers. For some, it’s about appetite feeling stronger or harder to control. For others, it’s how the body processes food, how full they feel after eating, or even how stress, sleep, and emotions influence eating habits. On top of that, the environment—like family routines, access to food, and daily activity—can shape things in a big way too.
Because of all this, treatment works better when it’s personalized instead of “one plan for everyone.” Some people benefit most from changes in food and activity, others may need extra medical support, and in some cases medication or surgery is considered. The goal isn’t just weight loss—it’s finding an approach that actually fits the person’s life and can be sustained long term.
What strikes me about applying phenotype-guided care to pediatric and adolescent obesity specifically is that we're trying to characterize a moving target. An adult's metabolic and behavioral phenotype tends to be relatively stable, but a fourteen-year-old's hunger signaling, activity patterns, and even family food environment can shift dramatically over a couple of years as they move through puberty, school transitions, and increasing autonomy over their own choices. That doesn't make phenotyping less valuable, but it does mean reassessment needs to happen far more frequently than it would in adult practice.
The piece I find most clinically actionable here is the family and environmental domain, because in pediatrics that's often the lever with the most leverage. A child's eating behaviors and activity levels are largely downstream of household structure, food access, and parental modeling, so even a precise phenotype assessment is only as useful as our ability to engage the family system around it. I think the future of pediatric obesity care will depend as much on building family-level intervention capacity as it will on matching the right pharmacologic or surgical tool to the right phenotype.
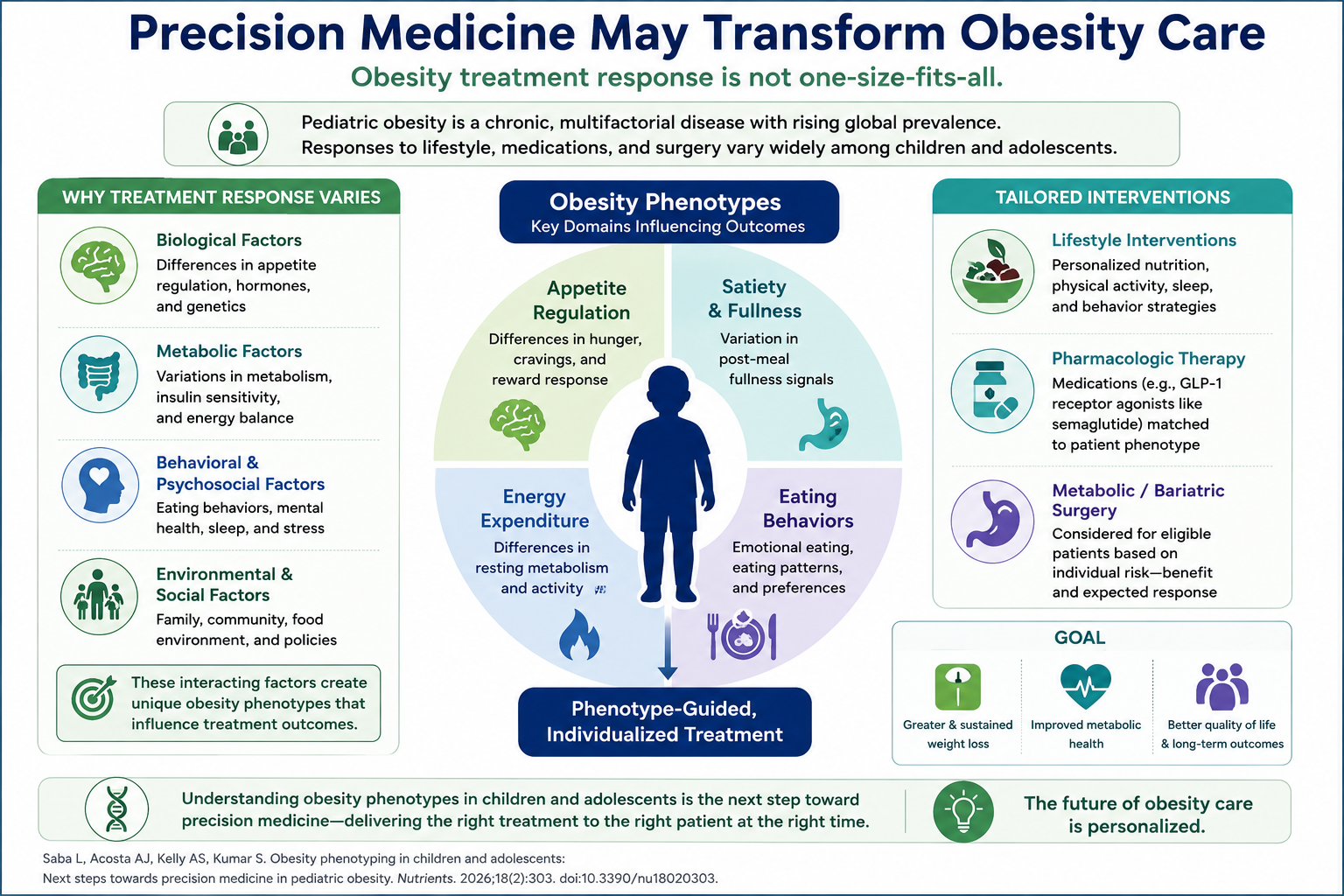
This infographic highlights the shift toward precision medicine in obesity care, recognizing that treatment response varies based on biological, metabolic, behavioral, and environmental factors. Phenotype-guided approaches that consider appetite regulation, satiety, energy expenditure, and eating behaviors may help match patients to the most appropriate lifestyle, pharmacologic, or surgical interventions.
The key message is that obesity is not a one-size-fits-all disease, and individualized treatment strategies may improve weight loss, metabolic health, and long-term outcomes by targeting the factors most relevant to each patient.
This infographic shows a major change in how we manage obesity: treating obesity as a heterogeneous, chronic disease, rather than a single disease with a particular response to treatment. Differences in appetite regulation, satiety signaling, energy expenditure, eating practices, genetics, metabolic health, and psychological factors may all contribute to the patients’ responses to lifestyle therapies, medication, or bariatric surgery.
In clinical practice a phenotype-guided strategy helps to promote more tailored treatment planning. Factors like as hunger patterns, emotional eating, sleep quality, physical activity, family environment and metabolic comorbidities should be assessed to identify the most relevant therapies for each patient. The aim is not merely a loss of weight, but lasting benefits in metabolic health, quality of life and long-term outcomes through individualised treatment.
This really highlights why the “one-size-fits-all” approach rarely works—obesity is shaped by a complex mix of biology, metabolism, behavior, and environment, especially in children and teens. Precision medicine that identifies individual phenotypes lets us move beyond generic advice to tailor lifestyle changes, medications, or surgical options to match each person’s unique needs. This shift not only improves the chance of meaningful, sustained weight loss but also boosts metabolic health and quality of life, while reducing frustration for both patients and providers. It’s a promising step forward in treating obesity as the chronic, diverse disease it truly is.
Obesity care should be personalized anyways for each individual person whether child, teenager, adult or the elderly. As stated above many factors influence obesity, social factors are huge because if a person grows up in a home where they only have access to certain foods or eat certain things culturally then this is a big issue that separates individuals and treatment plans like seeing a nutritionist to help navigate diet and find healthier alternatives to the foods the person is used too. Also things like mental disorders also should be addressed but this is another factor that can greatly impact obesity but can be tackled with CBT and potentially medications.
I have used Wegovy in adolescents with varied success. The biggest challenge is lifestyle modifications which are difficult to achieve in this population of patients
Start with family support structures, community food, access, and over eating regional policies. Eating behaves physical activities, sleep and stress factors, long-term behavior and structure routine habits building.
Childhood obesity rightly should be a focus. It is a complex issue and I feel it is important that medication not take the place of the need for intense lifestyle interventions. Medication may be appropriate for a few patients, but the majority require focused and ongoing nutritional and behavioral health support.




Because of all this, treatment works better when it’s personalized instead of “one plan for everyone.” Some people benefit most from changes in food and activity, others may need extra medical support, and in some cases medication or surgery is considered. The goal isn’t just weight loss—it’s finding an approach that actually fits the person’s life and can be sustained long term.
The piece I find most clinically actionable here is the family and environmental domain, because in pediatrics that's often the lever with the most leverage. A child's eating behaviors and activity levels are largely downstream of household structure, food access, and parental modeling, so even a precise phenotype assessment is only as useful as our ability to engage the family system around it. I think the future of pediatric obesity care will depend as much on building family-level intervention capacity as it will on matching the right pharmacologic or surgical tool to the right phenotype.
The key message is that obesity is not a one-size-fits-all disease, and individualized treatment strategies may improve weight loss, metabolic health, and long-term outcomes by targeting the factors most relevant to each patient.
In clinical practice a phenotype-guided strategy helps to promote more tailored treatment planning. Factors like as hunger patterns, emotional eating, sleep quality, physical activity, family environment and metabolic comorbidities should be assessed to identify the most relevant therapies for each patient. The aim is not merely a loss of weight, but lasting benefits in metabolic health, quality of life and long-term outcomes through individualised treatment.